In the acute phase after whiplash injury, most patients report pain and disability. Usually, these complaints reduce gradually within the first three months (1). Some patients continue to experience pain and disability and develop chronic Whiplash Associated Disorders (WAD). The proportion of patients developing a chronic condition diverges in literature from 20% up to 60%, depending on a variety of factors such as age, gender, ethnicity, and insurance system (2). Even without a detectable pathological lesion at physical examinations or imaging techniques, symptoms can remain. Current research shows that changes in the central processing of sensory input play an important role in the discrepancy between objective signs of tissue damage and complaints (3).
Although no gold standard is available to assess pain processing, Quantitative Sensory Testing (QST) is commonly utilized to track changes in the sensory system (4). This includes a composition of different techniques to assess the subjective response to stimulation of the somatosensory afferents in a controlled, graded, and physiological manner. The purpose of QST is to provide a detailed and reliable representation of pain processing.
Based on self-reported pain and disability, most individuals recover within the first three months. After this period, no big improvements occur and pain becomes chronic (1). The question arises if central pain processing outcomes, measured by QST, show a similar pattern. Marcuzzi et al. (5) concluded that thermal and widespread mechanical hypersensitivity is present within the first weeks after a whiplash trauma and persists in those who do not recover for at least three months. It is not clear how the somatosensory function evolves from the acute to and during the later phases. This is however crucially important in the understanding of the mechanisms involved in the development of chronic WAD. Therefore, we conducted a systematic review to search for studies that examine temporal changes in pain processing in WAD, measured by QST. Our systematic review summarized the current knowledge on adaptations in pain processing after whiplash injury and focused on the development over time. Thereby, we gained more clarity about the development of altered pain processing in the acute phase as well as throughout the years that follow. This review is not yet published, but this blog already gives some insight into the results (6).
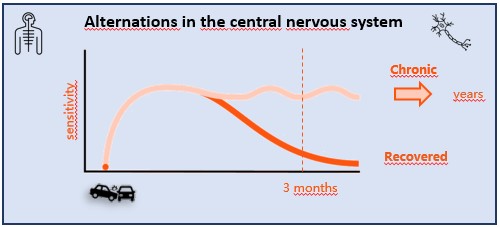
In general, results of the included studies show adaptations in the nociceptive pathways after whiplash trauma. These changes occur within the first month and seem to normalize during the second or third month in most patients. This normalization follows the principles and timeline of normal soft-tissue repair. However, in patients who eventually develop chronic disabling complaints, the somatosensory function remains disturbed for years after the injury. Moreover, by dividing the patients based on their recovery, differences in pain processing can already be seen in the early phase. In the acute stage, widespread mechanical hyperalgesia and primary thermal hyperalgesia were only present in the group that eventually developed chronic pain. These features can be considered as strong predictive factors for chronification.
This review highlights the importance of QST as a feasible and effective tool to identify patients at high risk to develop chronic complaints. The lack of improvements in the chronic stage pinpoints the need for early screening and treatment.
To conclude, differences in pain processing between patients that will recover and those that will develop chronic WAD can be observed already in the acute phase. Early screening for signs of altered pain processing can identify high risk patients, in order to prevent chronification. These insights into temporal changes show the importance of patient-tailored rehabilitation in the acute phase.
Jente Bontinck
2020Pain in Motion
References and further reading:
INCLUDED STUDIES IN THE REVIEW
Chien A, Eliav E, Sterling M. The development of sensory hypoesthesia after whiplash injury. Clinical Journal of 2010;26(8):722-728.
Daenen L, Nijs J, Cras P, Wouters K, Roussel N. Changes in Pain Modulation Occur Soon After Whiplash Trauma but are not Related to Altered Perception of Distorted Visual Feedback. Pain Pract 2014;14(7):588-598.
De Kooning M, Daenen L, Roussel N, Cras P, Buyl R, Ickmans K, Struyf F, Nijs J. Endogenous pain inhibition is unrelated to autonomic responses in acute whiplash-associated disorders. J Rehabil Res Dev 2015;52(4):431-440.
Dunne RL, Kenardy J, Sterling M. A randomized controlled trial of cognitive-behavioral therapy for the treatment of PTSD in the context of chronic whiplash. Clin J Pain 2012;28(9):755-765.
Kamper SJ, Rebbeck TJ, Maher CG, McAuley JH, Sterling M. Course and prognostic factors of whiplash: a systematic review and meta-analysis. Pain 2008;138(3):617-629.
Kasch H, Stengaard-Pedersen K, Arendt-Nielsen L, Jensen TS. Pain thresholds and tenderness in neck and head following acute whiplash injury: a prospective study. Cephalalgia 2001;21(3):189-197.
Kasch H, Hjorth T, Svensson P, Nyhuus L, Jensen TS. Temporomandibular disorders after whiplash injury: a controlled, prospective study. J Orofac Pain 2002;16(2):118-128.
Kasch H, Qerama E, Bach FW, Jensen TS. Reduced cold pressor pain tolerance in non-recovered whiplash patients: a 1-year prospective study. Eur J Pain 2005;9(5):561-569.
Kasch H, Qerama E, Kongsted A, Bach FW, Bendix T, Jensen TS. Deep muscle pain, tender points and recovery in acute whiplash patients: a 1-year follow-up study. Pain 2008;140(1):65-73.
Nebel K, Stude P, Ludecke C, Wiese H, Diener HC, Keidel M. Prospective PC-interactive pressure algesimetry of post-traumatic neck pain after whiplash injury. Cephalalgia 2005;25(3):205-213.
Olivegren H, Jerkvall N, Hagstrom Y, Carlsson J. The long-term prognosis of whiplash-associated disorders (WAD). Eur Spine J 1999;8(5):366-370.
Sterling M, Jull G, Vicenzino B, Kenardy J. Sensory hypersensitivity occurs soon after whiplash injury and is associated with poor recovery. Pain 2003;104(3):509-517.
Sterling M, Jull G, Kenardy J. Physical and psychological factors maintain long-term predictive capacity post-whiplash injury. Pain 2006;122(1-2):102-108.
Sterling M. Differential development of sensory hypersensitivity and a measure of spinal cord hyperexcitability following whiplash injury. Pain 2010;150(3):501-506.
{kind=link}
{kind=link}