Postmenopausal women with hormone receptor-positive breast cancer receive hormone therapy as part of their cancer treatment. One of the most frequently used and evidence-based hormone treatments are aromatase inhibitors (= inhibitors of the enzyme aromatase) that inhibit the conversion of androgens to estrogens. This results in decreased availability of estrogens and slowed progression of breast cancer.
So far the good news. Treatment adherence is low and drug discontinuation is high for these treatments. One of the main reasons for this is pain. Patients under hormonal therapy often suffer from pain: approximately 50% of breast cancer survivors on aromatase inhibitor therapy report musculoskeletal pain1. Alternatives like tamoxifen results in less severe pain and musculoskeletal symptoms as compared to aromatase inhibitor therapy (1).
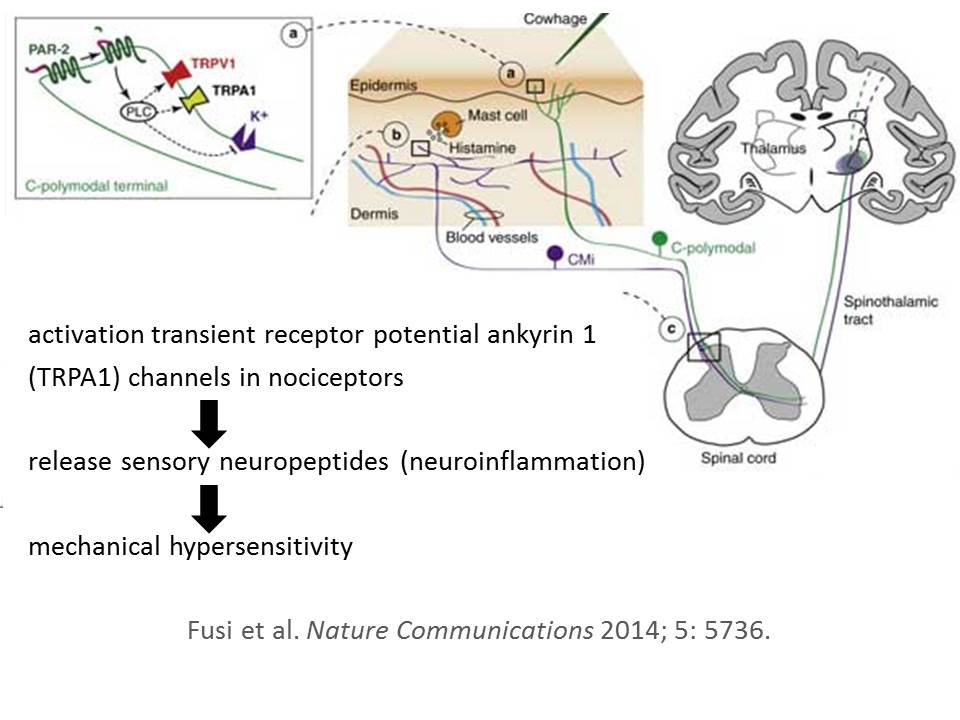
The reason for this common side effect of aromatase inhibitors is still an active area of research, and advances have been made. Recent animal work suggests that aromatase inhibitors selectively target the transient receptor potential ankyrin 1 (TRPA1) channel, a major pathway in pain transmission and neurogenic inflammation (2). Aromatase inhibitors activate TRPA1 channels in nociceptors, resulting in the release of sensory neuropeptides (i.e. neuroinflammation) and mechanical hypersensitivity (figure), together corresponding to a picture of generalized peripheral sensitization rather than nociception. TRPA1 is not only expressed on the distal, but also on the central endings of the primary afferent nociceptive fibers, located within the spinal dorsal horn (3). The latter finding points also to sensitization of central nervous system pathways, but further work is required to unravel the nature of aromatase inhibitors-induced pain.
In the meantime, patients continue to suffer from pain and deserve effective treatments. Providing analgesic drugs for the treatment of a side-effect of another drug is obviously not the preferred option. Therefore, Melinda Irwin and her colleagues from Yale University, University of Pennsylvania, Boston University and Colombia University (U.S.A.) have reported a sound randomized controlled trial showing that exercise therapy is effective in decreasing aromatase inhibitors-induced arthralgia in breast cancer survivors (4). The study is published in one of the leading journals in the field of oncology.
Exercise therapy comprised of a combination of aerobic and strengthening exercises. More specifically, breast cancer survivors performed a home-based aerobic exercise program of 150 minutes per week (walking or cycling) at 50 to 80% of maximal heart rate. The strength training included supervised resistance training of lower and upper limb muscles and was performed twice per week.
The control group received usual care and showed a slight pain increase troughout the study period. The treatment group improved markedly in pain severity and disability scores, with a mean improvement of 29% in pain severity 4. This number is most likely to reflect a clinically important improvement, but given the capacity of the placebo effect to generate large improvements in pain severity, a placebo-controlled trial with similar treatment time for both arms is required to confirms these compelling findings.
Taken together, this is one of the first high-quality trails regarding the treatment of aromatase inhibitor-induced arthralgia in breast cancer survivors. The study findings are important for clinical practice: exercise therapy is effective in reducing pain severity and disability in breast cancer survivors having aromatase inhibitor-induced arthralgia.
Jo Nijs
2015 © Pain in Motion
Reference and further reading:
1. Peppone LJ, Janelsins MC, Kamen C, et al. The effect of YOCAS(c)((R)) yoga for musculoskeletal symptoms among breast cancer survivors on hormonal therapy. Breast cancer research and treatment 2015; 150(3): 597-604.
2. Fusi C, Materazzi S, Benemei S, et al. Steroidal and non-steroidal third-generation aromatase inhibitors induce pain-like symptoms via TRPA1. Nature communications 2014; 5: 5736.
3. Pertovaara A, Koivisto A. TRPA1 ion channel in the spinal dorsal horn as a therapeutic target in central pain hypersensitivity and cutaneous neurogenic inflammation. Eur J Pharmacol 2011; 666(1-3): 1-4.
4. Irwin ML, Cartmel B, Gross CP, et al. Randomized exercise trial of aromatase inhibitor-induced arthralgia in breast cancer survivors. Journal of clinical oncology : official journal of the American Society of Clinical Oncology 2015; 33(10): 1104-11.
http://www.ncbi.nlm.nih.gov/pubmed/2545243
{kind=link}