Chronic musculoskeletal pain is a complex problem and has significant psychological, physical, social and economic implications. There is inevitable pressure for hospitals to reduce waiting times and improve treatment outcomes. Given the significant burden upon the individual, society and the economy, it is important to identify more effective management strategies.
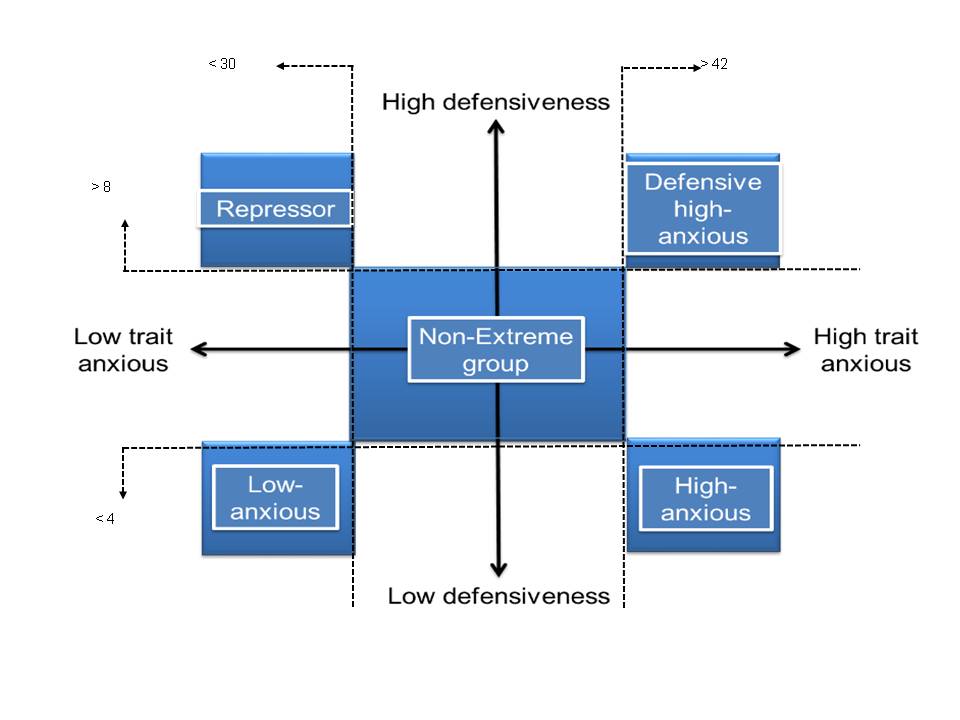
The majority of individuals will benefit from an interdisciplinary approach, which addresses different aspects of their pain simultaneously. Pain management programs (PMPs) are designed to address cognitive factors and to provide patients with management strategies in order to reduce their reliance upon healthcare services and improve function. Successful self-management can be difficult for some individuals while others appear able to effectively manage their condition at home. The mechanisms behind these differences between individuals are poorly understood, but have been suggested to be a function of personality type (Weinberger et al. 1979). The inclusion of defensiveness alongside trait anxiety (personality type, Figure 1) has highlighted differences in how individuals perceive pain and respond to treatment and health outcomes in chronic illness populations (Prasertsri et al. 2011). Recent research has found a significantly higher number of defensive high-anxious individuals within a chronic musculoskeletal pain population that that seen in the wider non-clinical population.
Figure 1. Diagram to demonstrate criterion splits of the four personality types.Through a series of studies, we highlighted important differences in the response to pain and pain management between the personality types, which are masked if the population is pooled and analysed homogenously. Within a dot probe study, defensive high-anxious individuals were shown to attend more to pain related information, compared to repressors who avoided pain images. This increased attention may make them susceptible to comorbid conditions (e.g. depression). Compared to the non-extreme group, levels of disability were more influenced by cognitive factors in defensive high-anxious individuals. Interestingly, a greater proportion of the defensive high-anxious group reported clinically important changes for both pain and disability compared to the non-extreme individuals at both three and six months post baseline.
These findings suggest that cognitive treatments are more effective for defensive high-anxious patients, however, these individuals continue to seek further treatment. The high proportion of defensive high-anxious individuals highlights the need for psychologically based interventions to be delivered earlier. Stratifying the population may allow for more targeted interventions, which could be more cost effective and reduce the number of patients remaining in the care system.
Zoe Franklin
Profile of Zoe Franklin
2015 Pain in Motion
References and further reading:
Franklin, Z.C., Smith, N.C. and Fowler, N.E. (2015) ‘Influence of defensiveness on disability in a chronic musculoskeletal pain population.’ Pain Practice. doi: 10.1111/papr.12337http://www.ncbi.nlm.nih.gov/pubmed/26179825
Franklin, Z.C., Smith, N.C. and Fowler, N.E. (2014) ‘Defensive high-anxious individuals with chronic back pain demonstrate different treatment choices and patient persistence.’ Personality and Individual Differences, 64 pp. 84-88. doi: http://dx.doi.org/10.1016/j.paid.2014.02.020
Prasertsri, N., Holden, J., Keefe, F. J. and Wilkie, D. J. (2011) 'Repressive coping style: Relationships with depression, pain, and pain coping strategies in lung cancer out patients.' Lung Cancer, 71(2) pp. 235-240.http://www.ncbi.nlm.nih.gov/pubmed/20557973
Weinberger, D. A., Schwartz, G. E. and Davidson, R. J. (1979) 'Low-anxious, high-anxious, and repressive coping styles: psychometric patterns and behavioral and physiological responses to stress.' Journal of Abnormal Psychology, 88(4) p. 369-380.http://www.ncbi.nlm.nih.gov/pubmed/479459
{kind=link}