Nociplastic pain may not be characterized only by sensory hypersensitivity. What about persistent, widespread pain with numbness and sensory loss or hypo-sensitivity? How do we classify people with no allodynia to light touch, stroking nor hot/cold applied to the skin, no hyperpathia nor temporal summation but with widespread, unpredictable pain, perhaps some weakness, fatigue, sleep dysfunction and/or cognitive difficulties? I regularly (about 30-40% of the time in my pain clinic) find that these individuals have pain that is not predominantly nociceptive nor neuropathic, and they fulfill all the current IASP (2021) criteria for a probable predominant nociplastic pain presentation, apart from the evoked pain hypersensitivity tests. Instead, the clinical sensory tests reveal sensory hypo-sensitivity to static and dynamic allodynia tests with no evidence of temporal summation nor hyperpathia.
This sensory hypo-sensitivity either appears in one region, such as a unilateral lumbar region or in many cases, it presents as widespread and commonly unilaterally, such as down the arm and the leg of the same side, on the painful side.
Studies to date have shown that sensory hypo-sensitivity is prevalent in fibromyalgia, complex regional pain syndrome, functional neurological disorder and whiplash associated disorders (Rehm et al. (2010), Egloff et al., (2012), Malfliet et al., (2015), Stone and Vermeulen, (2016)). The work of Egloff et al., (2012) demonstrated unilateral somatosensory hypo-sensitivity in individuals with fibromyalgia, chronic low back pain and chronic musculoskeletal pain syndrome after acute injury, using quantitative sensory testing. Previous authors (Mailis et al., 2003, Mailis-Gagnon and Nicholson, 2010, 2012) describe this phenomenon as non-dermatomal somatosensory deficits (NDSDs), defined as "unexplainable hypo-aesthesiae (e.g. to cutaneous or other sensory modalities) ipsilateral to the site of pain (or worse pain), which do not conform to the distribution of peripheral nerves or dermatomes" (Mailis-Gagnon and Nicholson, 2012; p. 1787).
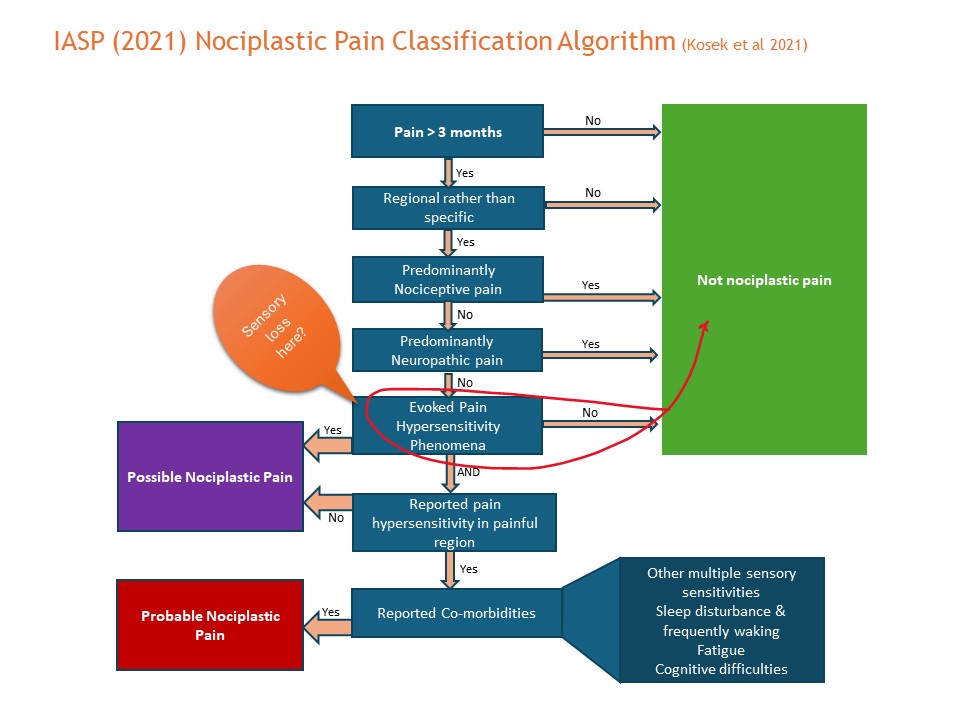
Using the current nociplastic pain classification criteria (IASP 2021), the group of persistent pain patients with sensory hypo-sensitivity, who do not test positive for allodynia and hyperpathia, would remain unclassified, just falling short at the “possible nociplastic pain” hurdle. See figure 1. Furthermore, they would remain unclassified even if the other criteria are met, i.e. reported pain hypersensitivity and co-morbidities associated with nociplastic pain (sleep dysfunction, frequent awakenings, fatigue and cognitive difficulties). This could lead to the individual remaining undiagnosed and untreated.
Why do some individuals develop NDSDs? On the basis that altered sensory processing is closely associated with nociplastic pain, one possible contributing factor to sensory loss, or NDSDs, is individual trait characteristics of sensory hypo-sensitivity to various sensory modalities (Brown et al., 2002), present pre-morbidly. Sensory hypo-sensitivity has been found in pre-pain populations such as those with neurodivergence (e.g. Bijlenga et al, 2017; Cadely, 2018), anxiety including those with self-harm tendencies (Cummins et al., 2021), and individuals with restless leg syndrome (Stiasne-Kolster et al., 2013). Trait (pre-morbid) sensory hypo-sensitivity has also been found to be a predictor of symptoms of central sensitization in chronic low back pain populations (Clark et al., 2019; Graper et al., submitted). There is a wide range of sensory sensitivity across general populations, a proportion of whom have genetically low pain- and sensory-sensitivity pre-morbidly (Diatchenko et al., 2005).
Other possible contributing factors for sensory hypo-sensitivity are psychological dissociative behaviors. Dissociation from the body part may be more likely to occur in post-trauma individuals, whether that be pre-morbid traumatic events or trauma inducing the inciting musculoskeletal pain. The individual may emotionally dissociate from the painful body part in association with a loss of sense of safety in the body, whereby sensory perception may become inhibited. The causes of sensory loss in individuals with non-neuropathic, non-nociceptive persistent pain still remain poorly understood.
Different treatment approaches are needed for individuals with NDSDs, compared to those with sensory hypersensitivity (Mailis et al, 2017). Key differences in non-pharmaceutical treatment approachesmay be based on the predominance of hypervigilance towards the painful area (as in sensory hypersensitivity) versus dissociative tendencies away from the painful area (as in sensory hypo-sensitivity). These clinical observations need further formal research investigation.
Conclusion
Sensory hypo-sensitivity in persistent pain conditions was first reported 20 years ago yet it is not acknowledged in the current nociplastic pain clinical classification algorithm. Many patients with non-nociceptive, non-neuropathic pain are remaining unclassified. Further research must be done to understand this phenomenon and work should progress towards inclusion of individuals with predominant sensory hypo-sensitivity, or NDSDs, in the nociplastic pain criteria. That way, the best course of treatment can be determined and it would avoid leaving individuals with non-nociceptive, non-neuropathic pain unclassified and out in the cold.
Dr Jacqui Clark
Jacqui Clark is a registered pain physiotherapy specialist in New Zealand. Her role includes clinical pain consultancy work, clinical mentoring for health care professionals, pain research and lecturing. She is a post doc researcher with VUB and a member of Pain in Motion since 2016.
2024Pain in Motion
References and further reading:
Brown, C., Cromwell, R. L., Filion, D., Dunn, W., & Tollefson, N. (2002). Sensory processing in schizophrenia: Missing and avoiding information. Schizophrenia research, 55(1-2), 187-195.
Bijlenga, D., Tjon-Ka-Jie, J. Y. M., Schuijers, F., & Kooij, J. J. S. (2017). Atypical sensory profiles as core features of adult ADHD, irrespective of autistic symptoms. European Psychiatry, 43, 51-57.
Cadely, F. A. (2018). Examining Orofacial Somatosensation Differences in Adults with and Without Adhd.
Clark, J. R., Nijs, J., Yeowell, G., Holmes, P., & Goodwin, P. C. (2019). Trait sensitivity, anxiety, and personality are predictive of central sensitization symptoms in patients with chronic low back pain. Pain Practice, 19(8), 800-810. https://www.sciencedirect.com/science/article/abs/...
Cummins, T. M., English, O., Minnis, H., Stahl, D., O’Connor, R. C., Bannister, K., . . . Ougrin, D. (2021). Assessment of somatosensory function and self-harm in adolescents. JAMA network open, 4(7), e2116853-e2116853.
Diatchenko, L., Slade, G. D., Nackley, A. G., Bhalang, K., Sigurdsson, A., Belfer, I., Goldman, D., Xu, K., Shabalina, S. A., Shagin, D., Max, M. B., Makarov, S. S. and Maixner, W. (2005) 'Genetic basis for individual variations in pain perception and the development of a chronic pain condition.' Human Molecular Genetics, 14(1) pp. 135-14. https://www.ncbi.nlm.nih.gov/pubmed/15537663
Egloff, N., Maecker, F., Stauber, S., Sabbioni, M. E., Tunklova, L. and von Känel, R. (2012) 'Nondermatomal somatosensory deficits in chronic pain patients: Are they really hysterical?' PAIN®, 153(9), 9//, pp. 1847-1851. https://www.ncbi.nlm.nih.gov/pubmed/22867972
Mailis-Gagnon, A. and Nicholson, K. (2010) 'Nondermatomal somatosensory deficits: overview of unexplainable negative sensory phenomena in chronic pain patients.' Current Opinion in Anesthesiology, 23(5): 593-7. https://www.ncbi.nlm.nih.gov/pubmed/20657277
Mailis-Gagnon, A. and Nicholson, K. (2012) ‘The paradox of less sensation and more pain’ Pain 153; 1787-1788. https://www.ncbi.nlm.nih.gov/pubmed/22658272
Mailis, A., & Nicholson, K. (2017). Nondermatomal Somatosensory Deficits (NDSDs) and Pain: State-of-the-Art Review. Psychological Injury and Law, 10(4), 313-329. doi:10.1007/s12207-017-9300-z
Malfliet, A., Kregel, J., Cagnie, B., Kuipers, M., Dolphens, M., Roussel, N., Meeus, M., Danneels, L., Bramer, W. M. and Nijs, J. (2015) 'Lack of evidence for central sensitization in idiopathic, non-traumatic neck pain: A systematic review.' Pain Physician, 18(3) pp. 223-235. https://www.ncbi.nlm.nih.gov/pubmed/26000666
Rehm, S. E., Koroschetz, J., Gockel, U., Brosz, M., Freynhagen, R., Tölle, T. R. and Baron, R. (2010) 'A cross-sectional survey of 3035 patients with fibromyalgia: subgroups of patients with typical comorbidities and sensory symptom profiles.' Rheumatology, 49(6) pp. 1146-1152. https://www.ncbi.nlm.nih.gov/pubmed/20236955
Stiasny-Kolster, K., Pfau, D. B., Oertel, W. H., Treede, R.-D., & Magerl, W. (2013). Hyperalgesia and functional sensory loss in restless legs syndrome. PAIN®, 154(8), 1457-1463.
Stone, J., & Vermeulen, M. (2016). Functional sensory symptoms. Handbook of clinical neurology, 139, 271-281. https://www.sciencedirect.com/science/article/abs/...
{kind=link}