Pain is the number one reason for patients visiting a physiotherapist. Chronic pain is the most costly condition affecting the Western world. This comes as no surprise: pain is omniprevalent among a wide variety of medical disciplines, ranging from oncology, pediatrics, geriatrics, rheumatology, orthopedics, neurology and internal medicine. For reducing the costs associated with chronic pain, correct mechanism-based classification of the pain type is the first step.
Most clinicians nowadays are aware of the possibility that pain can be either nociceptive or neuropathic in nature. Because the neuropathic pain criteria specify that a lesion or disease of the nervous system is identifiable and that pain is limited to a ‘neuroanatomically plausible’ distribution, they preclude the use of the term ‘neuropathic pain’ for people with widespread pain and nervous system sensitization (i.e. central sensitization pain). Such central sensitization pain implies that the central nervous system rather than peripheral damage dominates the patient’s clinical picture, and that pain results from hypersensitivity of the nervous system. Predominant central sensitization pain is present in many patients with whiplash associated disorders, headache, temporomandibular disorders, complex regional pain syndrome, fibromyalgia and chronic fatigue syndrome. A minority of patients with osteoarthritis, post-cancer pain, low back pain, shoulder pain, tennis elbow, chronic pelvic pain syndrome and many other chronic pain disorders also have predominant central sensitization pain. Yet clinicians were left wondering how to identify individuals having predominant central sensitization pain? This called for criteria defining central sensitization pain, or rather differentiating predominant central sensitization pain from neuropathic and nociceptive pain.
Therefore, a body of evidence from original research papers was used by 18 pain experts from seven different countries, including many Pain in Motion researchers/clinicians, to design the first classification criteria for central sensitization pain. In 2014, they proposed for the first time a set of classification criteria for central sensitization pain as an entity relatively distinct from other mechanisms-based classifications of pain such as neuropathic and nociceptive pain.
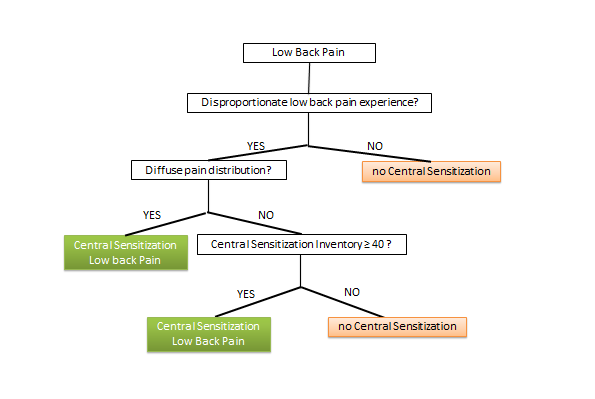
Although based on direct and indirect research findings, the classification algorithm requires experimental testing in future studies. Such studies are in progress. The proposed criteria allow clinicians to translate modern pain neuroscience into clinical practice, and many clinicians confirm that these criteria are a mainstay for mechanism-based classification of pain types in clinical practice. The Pain in Motion group acknowledges that every chronic pain population has its specificities, and therefore has started adopting these criteria for different groups of patients. The criteria for mechanism-based classification of low back pain patients in clinical practice are now available in Pain Physician journal, and they are working on a paper describing the complex case of post-cancer pain.
Further reading and free access to the full-text papers (PDF):
Applied to low back pain:
http://www.painphysicianjournal.com/2015/may/2015;18;E333-E346.pdf
Original criteria for serving clinicians:
http://www.painphysicianjournal.com/2014/september/2014;17;447-457.pdf
{kind=link}
{kind=link}