It is well known that pain is a complex phenomenon with challenging treatment. The Department of Health and Human Services recently published a National Pain Strategy, highlighting the insufficient training in pain assessment and treatment for many clinicians. Identifying the underlying mechanisms in the individuals’ pain experience can help in the choice of appropriate treatment. Although there is little agreement on how pain mechanisms can be classified in people with musculoskeletal pain (see blogpost “PAIN MECHANISMS: IS CONSENSUS ON TERMINOLOGY AND DEFINITION POSSIBLE? “ by Enrique Lluch), an interesting overview of a mechanism-based approach to physical therapy pain management was provided by Chimenti and colleagues (Chimenti, Frey-Law, & Sluka, 2018).
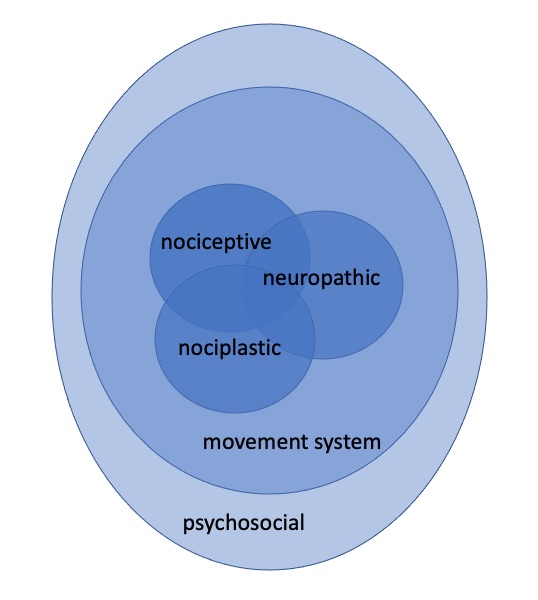
Pain is influenced by biological, psychosocial, and movement system factors, and according to the IASP (IASP, 2017) there are 3 types of(biological) pain mechanisms, including nociceptive, nociplastic, and neuropathic (Kosek et al., 2016; Phillips & Clauw, 2011). In order to apply a well-considered and mechanism-based approach, it is necessary to first evaluate for signs and symptoms suggestive of peripheral tissues and nociceptors (nociceptive), reduced central inhibition and/or enhanced central excitability (nociplastic), neuropathic pain signs and symptoms (neuropathic), psychological factors, and altered movement patterns.
According to the review, the following interventions may be applied when attempting to match treatments to the underlying pain mechanisms:
In conclusion: there is still much to learn about the underlying pain mechanisms and optimal interventions, yet significant advancements have occurred in the field of pain that are clinically relevant. Pain is no longer solely a peripherally driven symptom, and this framework can provide guidance to make educated treatment decisions that consider basic science and clinical effectiveness.
Lynn Leemans
2020Pain in Motion
References and further reading:
Chimenti, R. L., Frey-Law, L. A., & Sluka, K. A. (2018). A Mechanism-Based Approach to Physical Therapist Management of Pain. Phys Ther, 98(5), 302-314. doi:10.1093/ptj/pzy030
Sluka KA. Mechanisms and Management of Pain for the Physical Therapist. 2nd
ed. Seattle, WA: IASP Press; 2016
Max MB. Is mechanism-based pain treatment attainable? Clinical trial issues. J
Pain. 2000 Sep;1(3 Suppl):2-9. doi: 10.1054/jpai.2000.9819. PMID:
14622836.
International Association for the Study of Pain. Task Force on Taxonomy. IASP
Terminology. 2017. Available at: http://web.archive.org/web/20200130092932/https://...
Kosek, E., Cohen, M., Baron, R., Gebhart, G. F., Mico, J. A., Rice, A. S., . . . Sluka, A. K. (2016). Do we need a third mechanistic descriptor for chronic pain states? Pain, 157(7), 1382-1386. doi:10.1097/j.pain.0000000000000507
Phillips, K., & Clauw, D. J. (2011). Central pain mechanisms in chronic pain states--maybe it is all in their head. Best practice & research. Clinical rheumatology, 25(2), 141-154. doi:10.1016/j.berh.2011.02.005
{kind=link}