Several chronic musculoskeletal conditions are characterized by pain and changes in connective tissue. Treatment has traditionally focused on regional processes. Frequently, it is thought the injuries arise from a local origin. Herein, local inflammation initiates mechanisms to drive adaptation and repair. This response is followed by regenerative processes to restore normal tissue composition and function. However, in some of these conditions (e.g., low back pain, shoulder pain, complex regional pain syndrome), systemic inflammation has been found and might play a role in the development or persistence of the condition. In individuals with low back pain, shoulder pain, and complex regional pain syndrome, elevated levels of circulating pro-inflammatory cytokines were found (1, 2).
Under certain conditions, the ability of the body to clear injured tissue is impaired. Consequently, regulatory mechanisms are altered, and local inflammation becomes persistent and systemic. Another possibility for the development of systemic inflammation is that injury-repair cycles are too persistent for the complete resolution of inflammation. Next, inflammation can spread to include previously uninjured tissues. Unresolved systemic inflammatory responses may influence the inflammatory environment in otherwise uninjured tissues. Consequently, it may activate local inflammatory responses in the previously uninjured regions.
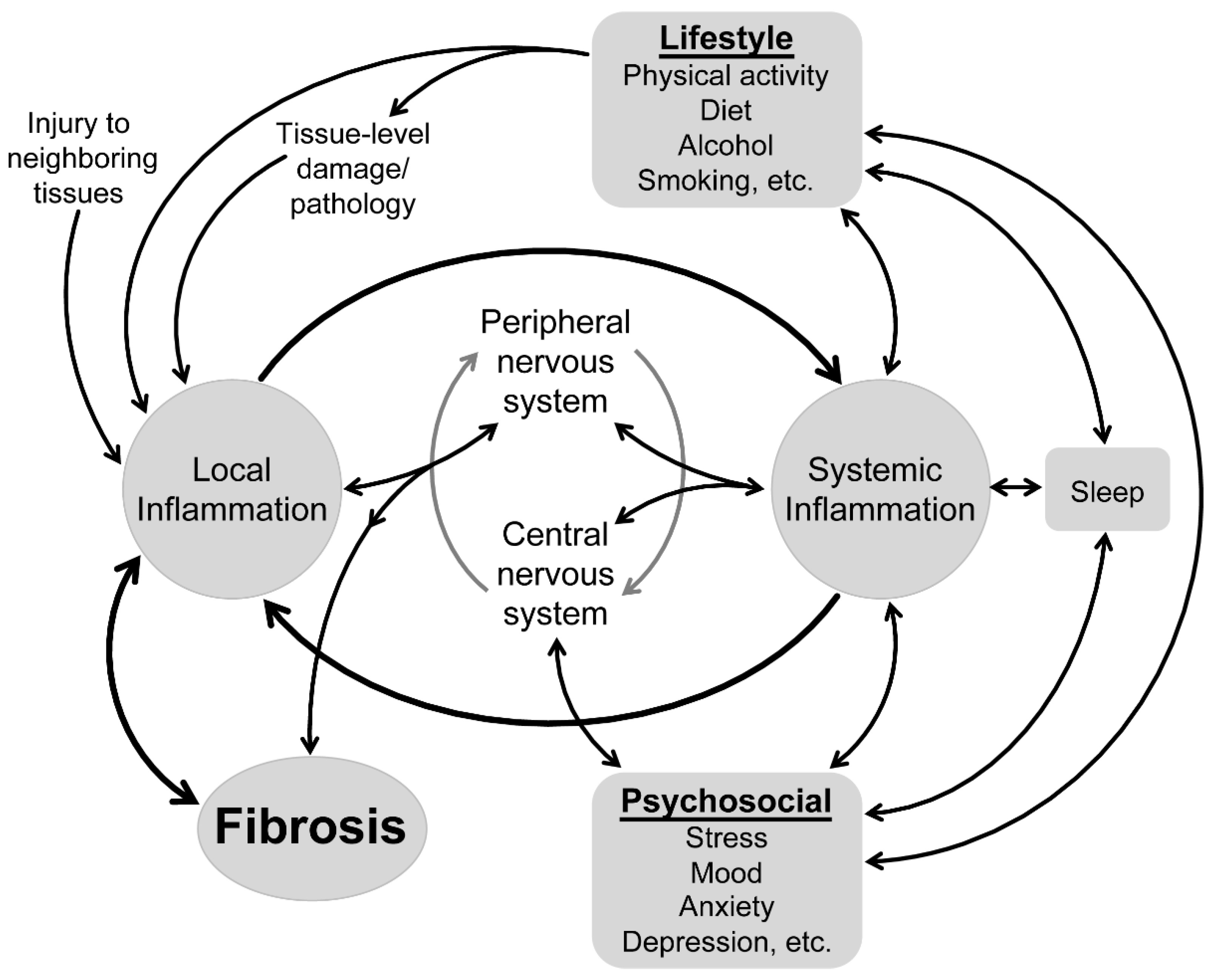
There is a bidirectional relationship between systemic and local inflammation. This relationship may provide an explanation for enhanced fibrosis in musculoskeletal tissues. Chronic muscle and tendon overuse induces increases in systemic levels of pro-inflammatory cytokines. Numerous inflammatory alterations have been observed in local tissue, including affected neighbouring tissue, but also in distant unrelated muscles. This highlights the potential influence of systemic mediators. Similar changes were found in non-musculoskeletal conditions. It appears that the inflammatory pathways in musculoskeletal and non-musculoskeletal conditions are similar.
Systemic inflammation may be present due to several factors. In musculoskeletal disorders an incomplete resolution of inflammation as a result of altered mechanisms regulating inflammatory responses or persistent injury repair cycles is one of them. Another factor might be comorbidities like diabetes mellitus and cardiovascular diseases. Systemic inflammation is frequently found in these comorbidities.
Systemic inflammation is linked to a range of psychosocial and lifestyle factors. It is suggested that psychosocial factors can disrupt the balance of the immune system and trigger a systemic inflammation. You can read more about the interaction between the immune and nervous system and external factors in one of my previous blogposts. One of the psychosocial factors influencing systemic inflammation is psychosocial stress. Stress and inflammation share similar pathways. They are both linked to the sympathetic nervous system and the hypothalamic pituitary adrenal (HPA)-axis. Activation of the sympathetic nervous system results in an upregulation of pro-inflammatory cytokines and consequently an increase in systemic inflammation. With recurrent or persistent stress, the function of the HPA-axis is altered (i.e., negative feedback regulation is altered) and immune cells become less sensitive to anti-inflammatory effects.
A lifestyle factor that has been found a well-known modulator of systemic inflammation is sleep. Sleep aids in the recovery from infections by regulating, among others, the sympathetic nervous system and the HPA-axis. Sleep disturbance can alter the inflammatory balance though activation of the stress response and/or inflammatory signalling pathways. Initially, this results in a shift in the temporal pattern of inflammatory responses, with increased levels of inflammatory cytokines during the day instead of during the night.
Other lifestyle factors linked to systemic inflammation are physical activity, alcohol use and cigarette smoke. Physical activity promotes anti-inflammatory processes, while inactivity promotes pro-inflammatory processes. Additionally, persistent inactivity leads to visceral adipose accumulation which is a potential source of inflammatory factors. Alcohol can induce inflammation via agents derived from alcohol damaged cells and derived from the gut microflora. Furthermore, heavy alcohol consumption increases gut permeability and can cause leakage of gut microflora-derived agents into the circulation and initiate an immune response. Besides alcohol, other foods can modulate inflammation via various mechanisms, including increased adiposity and gut permeability. Lasty, cigarette smoke is also a modulator of inflammation. Cigarette smoke modulates immunity that leads to inflammation.
Most of the inflammatory-related changes due to psychosocial and lifestyle factors are reversible. This emphasizes the importance to consider musculoskeletal disorders (including those with chronic pain) from a “whole system” perspective. This provides new opportunities to investigate the clinical relevance of interactions between inflammation, psychosocial and lifestyle factors, and innovative treatment programs in musculoskeletal conditions. For example, cognitive behavioural therapy applied to address insomnia can reduce systemic inflammatory activity and improvements in sleep are associated with reduced concentrations of circulating cytokines. If the management of sleep can reduce systemic inflammation, then it is plausible that that these inflammatory changes can also positively impact local inflammatory processes through systemic-to-local pathways. In this way local musculoskeletal conditions might benefit from a more general approach.
Michel GCAM Mertens
Graduate and research assistant University of Antwerp
2023 Pain in Motion
References and further reading: http://www.sciencedirect.com/science/article/pii/S...
This blogpost presents a summarized and simplified version of the hypotheses presented by Klyne et al. (unless stated otherwise). For more detail you can read the free full text:
Klyne DM, Barbe MF, James G and Hodges PW. Does the Interaction between Local and Systemic Inflammation Provide a Link from Psychology and Lifestyle to Tissue Health in Musculoskeletal Conditions? Int J Mol Sci 2021; 22: 7299. 20210707. DOI: 10.3390/ijms22147299.
Other references
1. Pietrzak M. Adhesive capsulitis: An age related symptom of metabolic syndrome and chronic low-grade inflammation? Medical hypotheses. 2016;88:12-7.
2. Stahnke K, Morawietz L, Moroder P, Scheibel M. Synovitis as a concomitant disease in shoulder pathologies. Archives of orthopaedic and trauma surgery. 2019;139(8):1111-6.
Free PDF available from:
{kind=link}