SYSTEMIC CYTOKINE LEVEL DIFFERENCES IN PATIENTS WITH CHRONIC MUSCULOSKELETAL SPINAL PAIN COMPARED TO HEALTHY CONTROLS AND ITS ASSOCIATION WITH PAIN SEVERITY
Chronic musculoskeletal pain is one of the most common chronic pain conditions and can be described as pain arising from muscles, tendons, joints and ligaments, which has been present for at least three months [1, 2]. Chronic spinal pain (CSP) is the most frequent form of chronic musculoskeletal pain and is situated in the cervical, thoracic or lumbar region [3-8]. Central hyperexcitability is responsible for common pain symptoms such as mechanical hyperalgesia, allodynia and widespread pain in chronic musculoskeletal pain [9, 10]. The cytokine signaling system is proposed as the underlying mechanism of central hyperexcitability [11-14]. Cytokines modulate perceived pain and contribute to the persistence of pain by acting in the spinal cord and brain [15]. Overflowing systemic cytokines can enter the spinal cord and the brain through, respectively, fenestrated vasculature, and the blood-brain barrier and circumventricular organ [16, 17]. Cytokines entering the spinal cord and brain eventually cause aberrant glial activation [16, 17]. Ultimately, these processes result in persistent pain [15, 18]. Based on these mechanisms, systemic cytokine assessment has been used to monitor pain severity for predicting recovery in CSP. However, this raises some questions: 1) Do differences exist in systemic cytokines in people suffering from CSP compared to healthy controls? 2) Are there any associations between systemic cytokines and pain severity in patients with CSP?
A recent study addressed these questions and reported the following results:
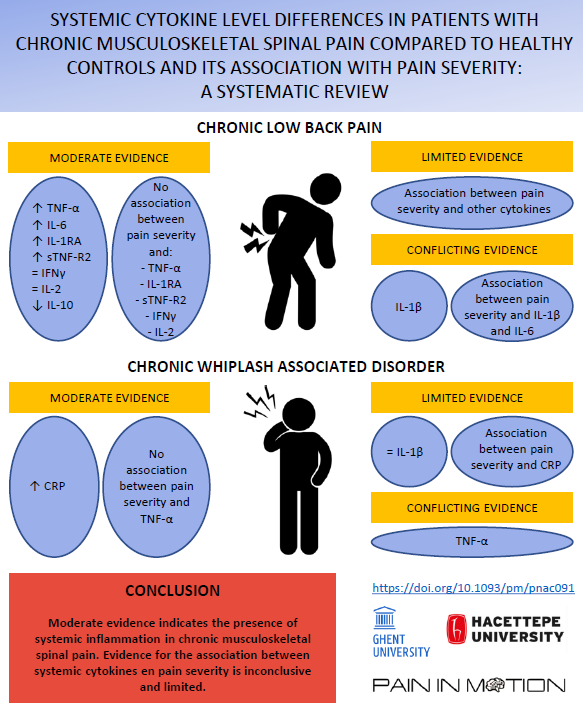
Chronic Low Back Pain (CLBP): In CLBP, moderate evidence indicates the presence of elevated TNF-α, IL-6, IL-1RA, and sTNF-R2, normal IFNγ and IL-2, and reduced IL-10 levels. Evidence on alterations in IL-1β levels in CLBP is inconclusive. Studying whether systemic cytokine levels are associated with pain severity, moderate evidence in CLBP showed that TNF-α, sTNF-R2, IFNγ, IL-2 and IL-1RA levels are not associated with pain severity. Furthermore, limited evidence supports a relation between serum CCL22, CCL20, CCL27, CX3CL1, CCL26, CCL19, CXCL13, and MIF levels and pain severity in CLBP. Evidence on the relation between IL-1β and IL-6 levels and pain severity in CLBP is inconclusive.
Chronic Whiplash Associated Disorder (CWAD): In CWAD, moderate evidence indicates the presence of elevated serum CRP levels, limited evidence points to normal serum IL-1β levels, and findings regarding changes in serum TNF-α levels are inconclusive. In CWAD, limited evidence indicates serum CRP levels to be associated with pain severity, while serum TNF-α levels do not seem to be associated with pain severity.
In conclusion, moderate evidence indicates the presence of systemic inflammation in CSP. Evidence regarding the association between pain severity and systemic cytokines is inconclusive and limited.
If you want to read more about the role of systemic cytokines in CSP, please follow the link:
https://academic.oup.com/painmedicine/advance-article-abstract/doi/10.1093/pm/pnac091/6608097
Amber Billens
Amber is a PhD student at Ghent University (Belgium) and conducts her research activities at the Department of Rehabilitation Sciences and Physiotherapy from Ghent University (Belgium) where she is a member of the Spine, Head and Pain Research Unit Ghent. Furthermore, she is a member of the Pain in Motion international research group. Her education exists of a Master of Science in Rehabilitation Sciences and Physiotherapy with specialization in musculoskeletal disorders and pediatrics.
Kübra Canlı
Kübra is a PhD student at the Physical Therapy and Rehabilitation Faculty at Hacettepe University (Turkey). Her interests are in the fields of neuroscience and musculoskeletal pain.
2022Pain in Motion
References and further reading:
[1] Treede RD, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain 2019;160(1): 19-27.
[2] Nicholas M, Vlaeyen JWS, Rief W, et al. The IASP classification of chronic pain for ICD-11: chronic primary pain. Pain 2019;160(1): 28-37.
[3] Manchikanti L, Staats PS, Singh V, et al. Evidence-based practice guidelines for interventional techniques in the management of chronic spinal pain. Pain Physician 2003; 6: 3-81. 2006/08/01.
[4] Côté P, Cassidy DJ, Carroll LJ, et al. The annual incidence and course of neck pain in the general population: a population-based cohort study. Pain 2004; 112: 267-273. 2004/11/25.
[5] Gerhardt A, Hartmann M, Blumenstiel K, et al. The prevalence rate and the role of the spatial extent of pain in nonspecific chronic back pain--a population-based study in the south-west of Germany. Pain Med 2014; 15: 1200-1210. 2013/12/18.
[6] Hoy D, Bain C, Williams G, et al. A systematic review of the global prevalence of low back pain. Arthritis Rheum 2012; 64: 2028-2037. 2012/01/11.
[7] Briggs AM, Smith AJ, Straker LM, et al. Thoracic spine pain in the general population: prevalence, incidence and associated factors in children, adolescents and adults. A systematic review. BMC Musculoskelet Disord 2009; 10: 77. 2009/07/01.
[8] Devereaux MW. Anatomy and examination of the spine. Neurol Clin 2007; 25: 331-351. 2007/04/21.
[9] Woolf CJ. Central sensitization: implications for the diagnosis and treatment of pain. Pain 2011;152(3 Suppl): S2-s15.
[10] Roussel NA, Nijs J, Meeus M, Mylius V, Fayt C, Oostendorp R. Central sensitization and altered central pain processing in chronic low back pain: fact or myth? Clin J Pain 2013;29(7): 625-38.
[11] Gonçalves Dos Santos G, Delay L, Yaksh TL, et al. Neuraxial Cytokines in Pain States. Front Immunol 2019; 10: 3061. 2020/02/13.
[12] Sterling M, Elliott JM and Cabot PJ. The course of serum inflammatory biomarkers following whiplash injury and their relationship to sensory and muscle measures: a longitudinal cohort study. PLoS One 2013; 8: e77903. 2013/10/23.
[13] Xue H, Yao Y, Wang X, et al. Interleukin-21 Is Associated with the Pathogenesis of Lumbar Disc Herniation. Iran J Allergy Asthma Immunol 2015; 14: 509-518. 2016/01/09.
[14] Teodorczyk-Injeyan JA, Triano JJ and Injeyan HS. Nonspecific Low Back Pain: Inflammatory Profiles of Patients With Acute and Chronic Pain. Clin J Pain 2019; 35: 818-825. 2019/07/10.
[15] Woolf CJ. Central sensitization: implications for the diagnosis and treatment of pain. Pain 2011; 152: S2-s15. 2010/10/22.
[16] Banks WA. The blood-brain barrier in psychoneuroimmunology. Immunol Allergy Clin North Am 2009;29(2): 223-8.
[17] Banks WA, Kastin AJ, Broadwell RD. Passage of cytokines across the blood-brain barrier. Neuroimmunomodulation 1995;2(4): 241-8.
[18] Nijs J, Loggia ML, Polli A, et al. Sleep disturbances and severe stress as glial activators: key targets for treating central sensitization in chronic pain patients? Expert Opin Ther Targets 2017; 21: 817-826. 2017/07/08.
{kind=link}