Acute pain is common in children
Acute pain is “a normal, predicted physiological response and experience to a noxious chemical, thermal or mechanical stimulus associated with acute illness, trauma or surgery”.1,2 Acute pain is usually sudden in onset, limited in time, and motivates behavioral responses to avoid actual or potential tissue damage.3 Cross-sectional studies report that 54-88% of children experienced at least one pain episode in the preceding 3 months.4-7 Relatively brief, mild to moderately intense, injury-related pain experiences are the most common acute pains in children.8,9 Another typical kind of acute pain is procedural pain10, which is commonly experienced at emergency and outpatient departments.
Undertreatment of pain has been frequently reported, particularly in younger children, children with cognitive impairment, and children in developing countries. Initiatives of the past decade include recording of pain scores, staff education, and quality improvement processes.11-14 Such efforts have fostered advances in the pharmacological and non-pharmacological treatment of pain in children.
Language as part of non-pharmacological acute pain management
In a previous blogpost, we discussed various non-pharmacological tips and tricks to minimize pain and distress during needle procedures in children. Complementary to these non-pharmacological approaches, we would like to share some interesting insights from Dr. Baruch S Krauss et al. (2016)15 about the importance of the words parents and health care providers use when talking to children in the context of acute pain.
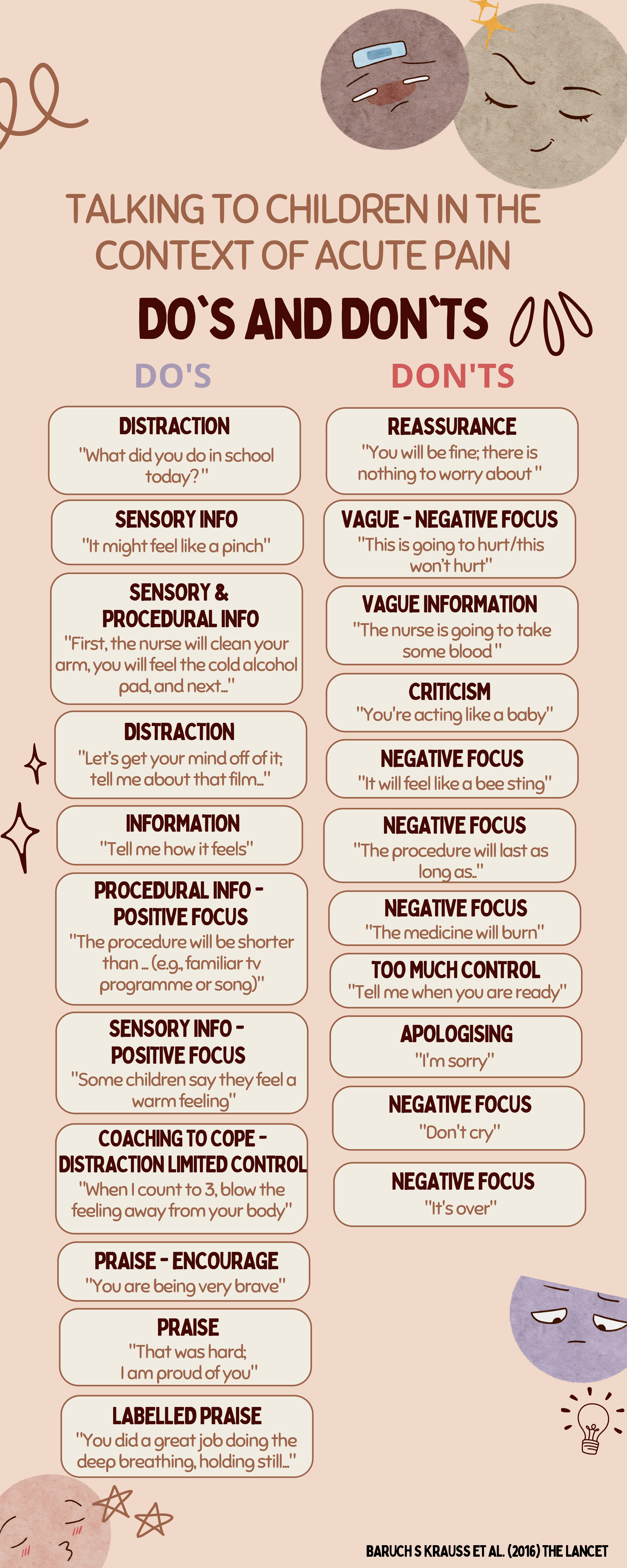
As an example, many parents, in an attempt to minimize their child’s anxiety and increase coping capability, will tell the child that he/she will be getting a small needle and that the procedure will only hurt for a minute. Despite the fact that these words are obviously well-intentioned and only aim to support the child as best as possible, it can backfire and increase pain and distress in the child. Therefore, it is recommended that parents are being prepared and coached. Clinicians can discuss with parents, before the examination or procedure and out of the child’s earshot, what will happen and how the parents can help their child to cope well. An important part of parent coaching, is to instruct them in the use of language-based coping skills (i.e., the use of developmentally specific words and phrases, encouragement, praise) and distraction activities and to avoid vague or negatively focused language, apology, global reassurance, criticism, or the use of potentially frightening terms.16,17 Assignment of these tasks to parents serves as a distraction for themselves, probably decreasing their personal anxiety that they, in turn, might transmit to their child. Words or phrases that are helpful to one child might be threatening to another, hence parents and health care providers should select their language carefully.16
Please check out this overview of do’s and don’ts when talking to children in the context of acute pain experiences, applying to both parents and health care providers.
A pdf version of this overview can be sent to you upon request via emma.rheel@vub.be.
Dr. Emma Rheel
Postdoctoral research at the Pain in Motion (PAIN) research group, Department of Physiotherapy, Human Physiology and Anatomy of the Vrije Universiteit Brussel, Brussels, Belgium
2023Pain in Motion
References and further reading:
[1] Carr DB, Goudas LC. Acute pain. The Lancet 1999; 353(9169): 2051-8. https://pubmed.ncbi.nlm.nih.gov/10376632/
[2] The Federation of State Medical Boards of The United States, Inc. Model guidelines for the use of controlled substances for the treatment of pain. S D J Med 1999; 52(1): 25-7. https://pubmed.ncbi.nlm.nih.gov/9926729/
[3] Tighe P, Buckenmaier CC, 3rd, Boezaart AP, et al. Acute Pain Medicine in the United States: A Status Report. Pain Med 2015; 16(9): 1806-26. https://pubmed.ncbi.nlm.nih.gov/26535424/
[4] Perquin CW, Hazebroek-Kampschreur A, Hunfeld JAM, et al. Pain in children and adolescents: a common experience. Pain 2000; 87(1): 51-8. https://pubmed.ncbi.nlm.nih.gov/10863045/
[5] Haraldstad K, Sørum R, Eide H, Natvig GK, Helseth S. Pain in children and adolescents: prevalence, impact on daily life, and parents' perception, a school survey. Scand J Caring Sci 2011; 25(1): 27-36. https://pubmed.ncbi.nlm.nih.gov/20409061/
[6] Roth-Isigkeit A, Thyen U, Raspe HH, Stöven H, Schmucker P. Reports of pain among German children and adolescents: an epidemiological study. Acta Paediatr 2004; 93(2): 258-63. https://pubmed.ncbi.nlm.nih.gov/15046285/
[7] Huguet A, Miró J. The severity of chronic pediatric pain: an epidemiological study. J Pain 2008; 9(3): 226-36. https://pubmed.ncbi.nlm.nih.gov/18088558/
[8] McGrath PA. Pain in Children: Nature, Assessment, and Treatment.: Guilford Press; 1990.
[9] van Dijk A, McGrath P, Pickett W, VanDenKerkhof EG. Pain prevalence in nine- to 13-year-old schoolchildren. Pain Res Manag 2006; 11(4): 234-40. https://pubmed.ncbi.nlm.nih.gov/17149456/
[10] Birnie KA, Noel M, Chambers CT, Uman LS, Parker JA. Psychological interventions for needle-related procedural pain and distress in children and adolescents. Cochrane Database Syst Rev 2018; 10(10): Cd005179. https://pubmed.ncbi.nlm.nih.gov/30284240/
[11] Boyd RJ, Stuart P. The efficacy of structured assessment and analgesia provision in the paediatric emergency department. Emerg Med J 2005; 22: 30–32. https://pubmed.ncbi.nlm.nih.gov/15611538/
[12] Eisen S, Amiel K. Introduction of a paediatric pain management protocol improves assessment and management of pain in children in the emergency department. Arch Dis Child 2007; 92: 828–29. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC20840...
[13] Somers LJ, Beckett MW, Sedgwick PM, Hulbert DC. Improving the delivery of analgesia to children in pain. Emerg Med J 2001; 18: 159–61. https://pubmed.ncbi.nlm.nih.gov/11354201/
[14] Todd KH, Ducharme J, Choiniere M, et al, and the PEMI Study Group. Pain in the emergency department: results of the pain and emergency medicine initiative (PEMI) multicenter study. J Pain2007; 8: 460–66. https://pubmed.ncbi.nlm.nih.gov/17306626/
[15] Krauss BS, Calligaris L, Green SM, Barbi E. Current concepts in management of pain in children in the emergency department. Lancet. 2016;387(10013):83-92. https://pubmed.ncbi.nlm.nih.gov/26095580/
[16] Cohen LL. Behavioral approaches to anxiety and pain management for pediatric venous access. Pediatrics 2008; 122 (suppl 3): S134–39. https://pubmed.ncbi.nlm.nih.gov/18978007/
[17] Kuttner L. A child in pain. Wales: Crown House Publishing, 2010.
{kind=link}