Around six years ago, I went to Kisumu, Kenya for an International Aid and Development program (IAD). My landlord there shared an educational story in the field of IAD. “Once upon a time”, she said, “an American engineer found out that women in Kisumu needed to walk for hours to get fresh water and carry that water back home. It was time-consuming and physical. Therefore, the engineer built a reservoir for water and people could get fresh water easily from the reservoir. However, the engineer found out later that these women still stuck to their original, inefficient route. Those women later explained that the time they spent on getting water was the only moment that they could take a break from their family and it was the chatting moment, a way of socializing with other women. ”
I constantly think about this story when I am doing my current research project - cultural adaptation of pain neuroscience education (PNE) for the Chinese chronic low back pain (LBP) population in physiotherapeutic settings. Documented as the second highest health burden since 1990, LBP has become a major concern within the field of Chinese health care (1). Growing evidence globally results in a shift in LBP management from a biomedical to a biopsychosocial view (2, 3). However, Chinese LBP care seems to be based on the biomedical model. The guidelines for LBP from the Chinese Association for the Study of Pain and the Chinese Association of Rehabilitation Medicine continuously view LBP as a biomedical problem (4-6). In line with those guidelines, an enormous misuse of diagnostic imaging of LBP has also been reported in China which might further imply the biomedical thinking in Chinese LBP practice (7). Pain neuroscience education (PNE) is an evidence-based intervention (8), having structuralized steps to help clinicians discuss biopsychosocial dimensions of pain and promote active coping strategies together with patients (9, 10). It has been used in physiotherapy practice for the management of chronic pain (11, 12). Therefore, PNE might also be useful to narrow the gap in psychosocial aspects of LBP care in China.
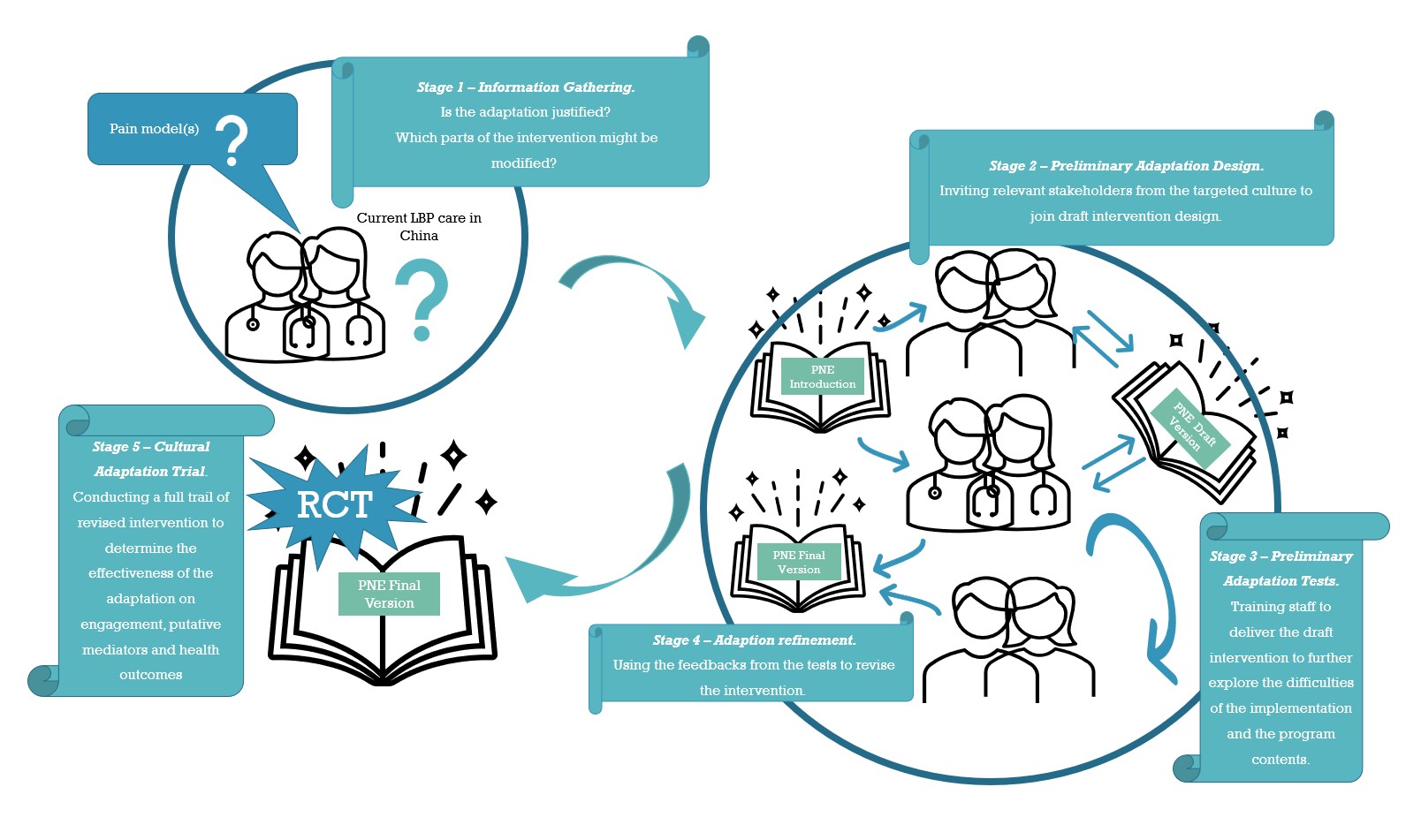
However, how can we avoid building a “water reservoir” during the process of introducing PNE to Chinese physiotherapeutic LBP care? Are Chinese physiotherapists satisfied with the current intervention they provide and are Chinese chronic LBP patients satisfied with the interventions they receive? Do therapists and LBP patients feel the need of PNE in current LBP care? What do they think about the original contents of PNE and what is the best way to apply PNE in their opinion? Answers to those questions need to be explored before introducing a brand new intervention to the current Chinese LBP care process (building a water reservoir directly). Luckily, Barrera et al., 2013 provided a five-stage framework to guide the cultural adaptation process of evidence-based interventions (13). From my perspective, it highlights the importance of systematically adapting an evidence-based intervention by carefully exploring the target context that influences the intervention implementation and the people involved. The key features of the five stages are listed in the picture.
Based on the framework (13), we plan to conduct two qualitative and one quantitative study as follows:
1) Study 1: Conduct in-depth and semi-structured individual interviews to explore Chinese physiotherapists’ understanding about pain and current physiotherapeutic LBP care. We will account the interview results into our preliminary PNE program.
2) Study 2: Organize focus groups and pilot tests with Chinese physiotherapists and chronic LBP patients, to discuss and test our preliminary PNE program. The results will be incorporated in the final construct of the PNE program.
3) Study 3: Perform a randomized controlled trial to assess the PNE program’s effectiveness on disability (primary outcome), pain, illness perceptions, pain catastrophizing, kinesiophobia and self-efficacy in Chinese chronic LBP patients.
Hopefully, we can share our interesting findings soon.
YiJun Li
PhD student at Vrije Universiteit Brussel and Hogeschool Rotterdam
2023 Pain in motion
References and further reading:
If you want to read more about the thinking patterns of pain causes in Chinese chronic LBP patients, please access my previous research: Li Y, Coppieters MW, Setchell J, Hodges PW, Scholten-Peeters GG. How do people in China think about causes of their back pain? A predominantly qualitative cross-sectional survey. BMC musculoskeletal disorders. 2020 Dec;21(1):1-1.
1. Wu A, Dong W, Liu S, Cheung JPY, Kwan KYH, Zeng X, et al. The prevalence and years lived with disability caused by low back pain in China, 1990 to 2016: findings from the global burden of disease study 2016. Pain. 2019;160(1):237-45.
2. Hartvigsen J, Hancock MJ, Kongsted A, Louw Q, Ferreira ML, Genevay S, et al. What low back pain is and why we need to pay attention. The Lancet. 2018;391(10137):2356-67.
3. Foster NE, Anema JR, Cherkin D, Chou R, Cohen SP, Gross DP, et al. Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet. 2018;391(10137):2368-83
4. Ma K, Zhuang Z-G, Wang L, Liu X-G, Lu L-J, Yang X-Q, et al. The Chinese Association for the Study of Pain (CASP): consensus on the assessment and management of chronic nonspecific low back pain. Pain Research and Management. 2019;2019.
5. 王祥瑞, 冯智英, 张小梅, 张洪新, 林建, 郑拥军, et al. 腰椎间盘突出症诊疗中国疼痛专家共识. 中国疼痛医学杂志. 2020;26(1):2-6.
6. 陈伯华, 陈其昕, 陈允震, 冯世庆, 黄东生, 姜建元, et al. 中国急/慢性非特异性腰背痛诊疗专家共识. 中国脊柱脊髓杂志. 2016;26(12).
7. Yu L, Wang X, Lin X, Wang Y. The Use of Lumbar Spine Magnetic Resonance Imaging in Eastern China: Appropriateness and Related Factors. PLoS One. 2016;11(1):e0146369.
8. Watson JA, Ryan CG, Cooper L, Ellington D, Whittle R, Lavender M, et al. Pain Neuroscience Education for Adults With Chronic Musculoskeletal Pain: A Mixed-Methods Systematic Review and Meta-Analysis. J Pain. 2019;20(10):1140.e1-.e22.
9. Butler DS, Moseley GL. Explain Pain; 2013.
10. Nijs J, van Wilgen P. Pijneducatie: een praktische handleiding voor (para) medici: Bohn Stafleu van Loghum; 2010.
11. Louw A, Puentedura EJ, Zimney K, Schmidt S. Know Pain, Know Gain? A Perspective on Pain Neuroscience Education in Physical Therapy. J Orthop Sports Phys Ther. 2016;46(3):131-4.
12. Wijma AJ, van Wilgen CP, Meeus M, Nijs J. Clinical biopsychosocial physiotherapy assessment of patients with chronic pain: The first step in pain neuroscience education. Physiother Theory Pract. 2016;32(5):368-84.
13. Barrera M, Jr., Castro FG, Strycker LA, Toobert DJ. Cultural adaptations of behavioral health interventions: a progress report. J Consult Clin Psychol. 2013;81(2):196-205.
{kind=link}