The scapula plays an important role in the function of the shoulder. During humeral elevation of the arm, a complex scapular movement of upward rotation, posterior tilt and external rotation is needed to create a stable base for the glenohumeral joint. The quality of this scapular movement depends on the coordinated activity of the surrounding superficial (trapezius and serratus anterior) and deeper (pectoralis minor, levator scapulae and rhomboid major) lying scapulothoracic muscles.
A lack of activation or excessive activation of scapulothoracic muscles may impede optimal scapular movement. One of the musculoskeletal pain disorders in which scapular movement is comprised is the shoulder impingement syndrome (SIS). The SIS symptoms are mostly present when the arm is elevated or when overhead activities are performed. During these type of movements a lack of upward and external rotation and posterior tilting of the scapula has been observed in SIS (reviewed by Struyf et al. 2011). Hence, it could be assumed that that recruitment of the muscles, which are responsible for this movement, is possibly altered in SIS.
To date, most studies that have investigated whether scapulothoracic muscle activity during humeral elevation is altered in patients with SIS have examined the superficial muscles using surface electromyography. Deeper lying muscles can also be investigated using electromyography, but require a more invasive methodology as fine wire electrodes need to be placed in the muscle using a needle. However, the information gathered using this technique is indispensable as deeper lying muscles are usually of great importance for the performance of movement in a controlled way.
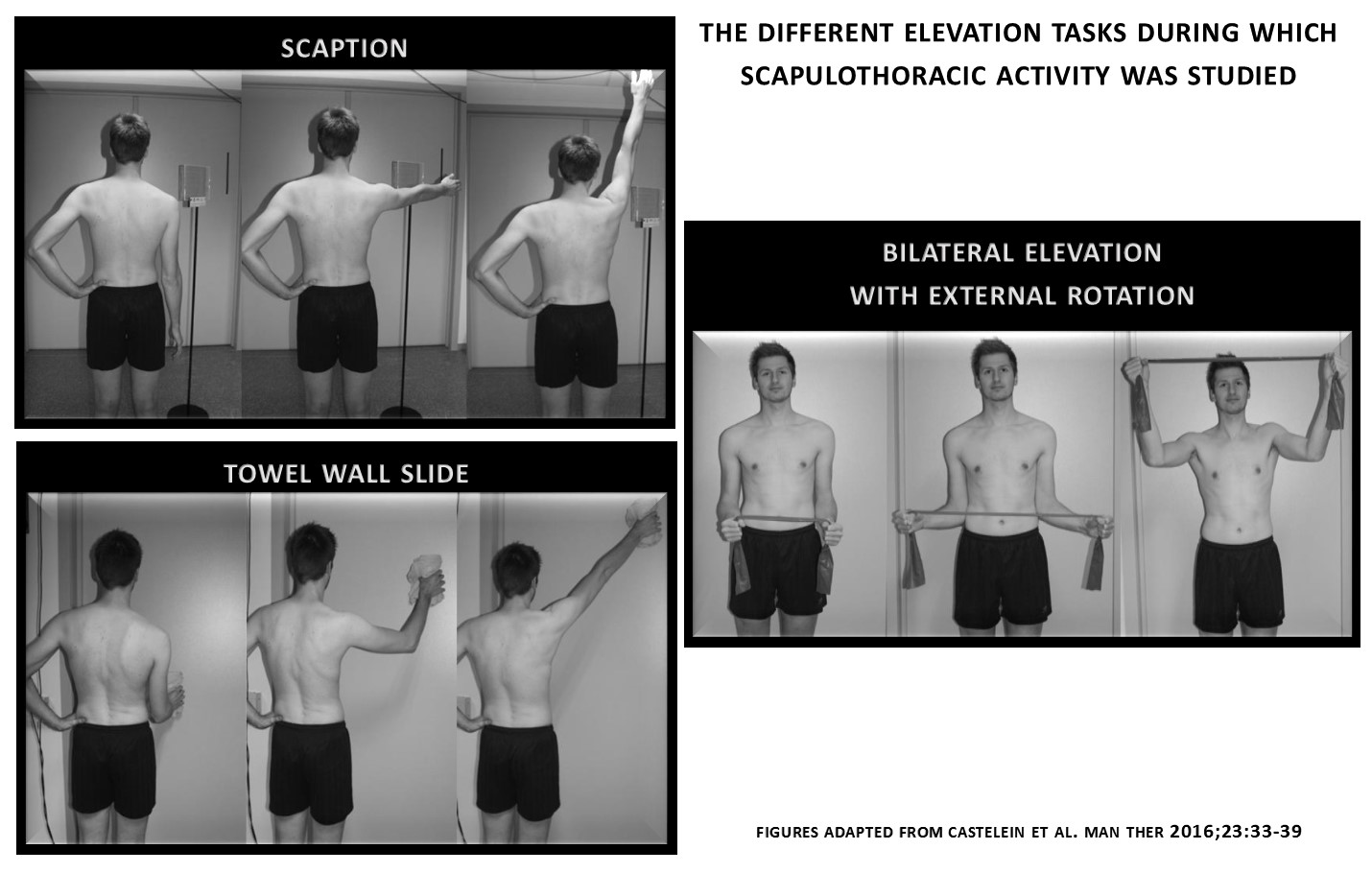
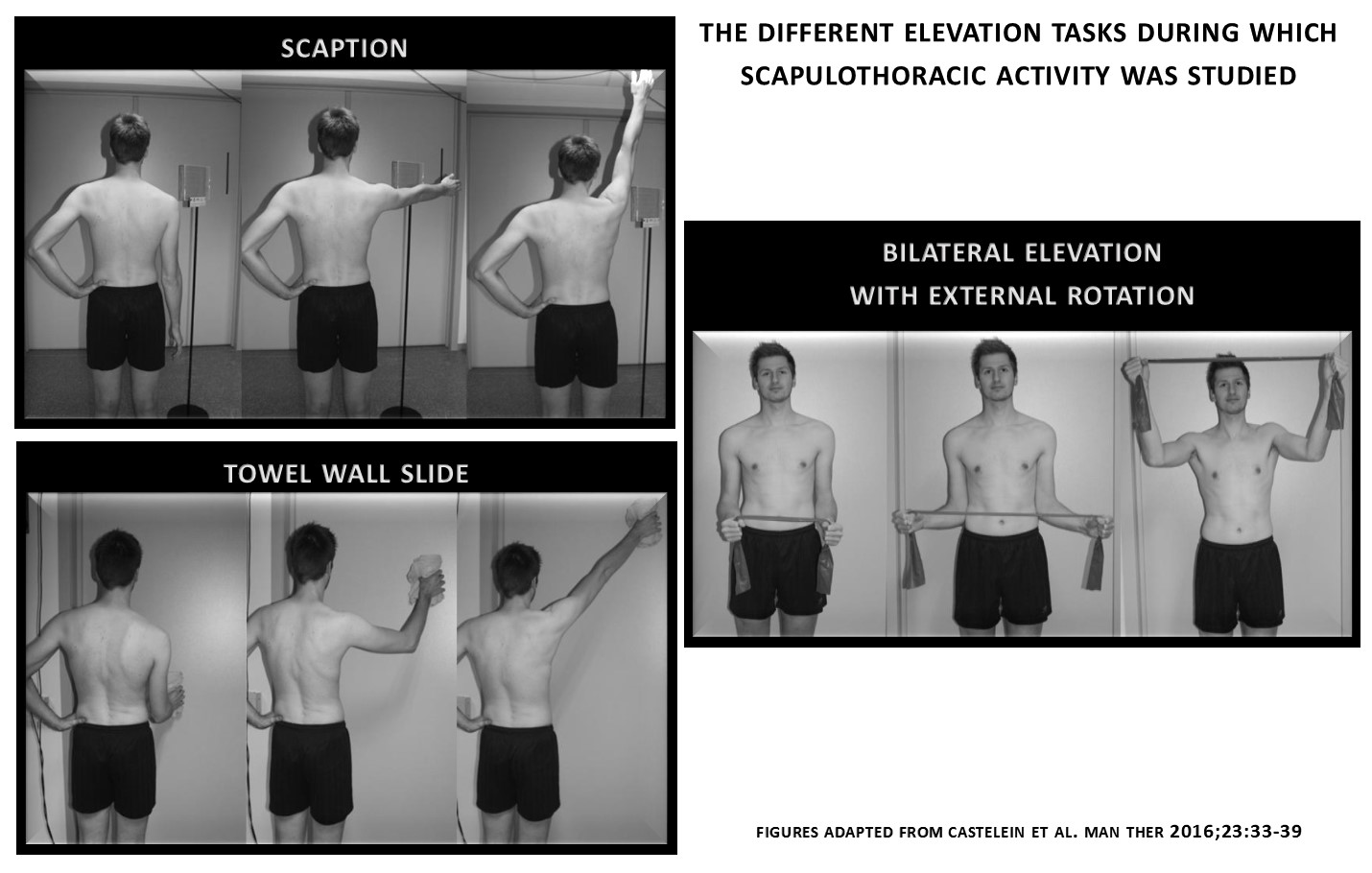
In this prospect, Castelein et al. 2016 decided to examine these muscles in SIS patients during different elevation tasks, namely elevation in the scapular plane, elevation during a towel slide against a wall, and elevation during external rotation using a theraband. Results were compared to a matched healthy control group. An overactive pectoralis minor was observed in the SIS patients, and this was the case during all the different elevation tasks. All other muscles functioned similar to those in the healthy group, indicating that the dysfunction of the pectoralis minor is key during elevation in SIS. It is believed that the extensibility of the pectoralis minor is affected and that this shortening and increased tension of the muscle explains the previous described malalignment of the scapula during elevation of the arm which in turn could lead to reduced subacromial space and thus the SIS symptoms.
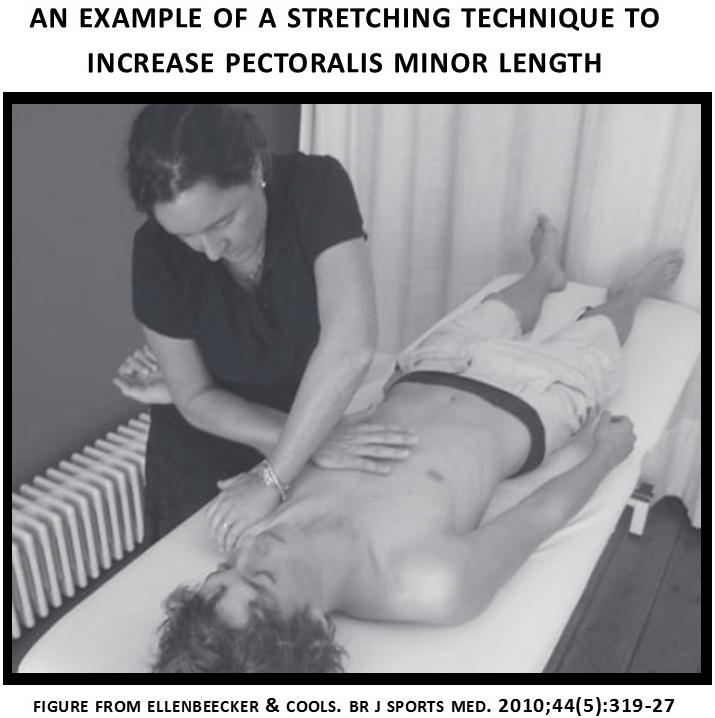
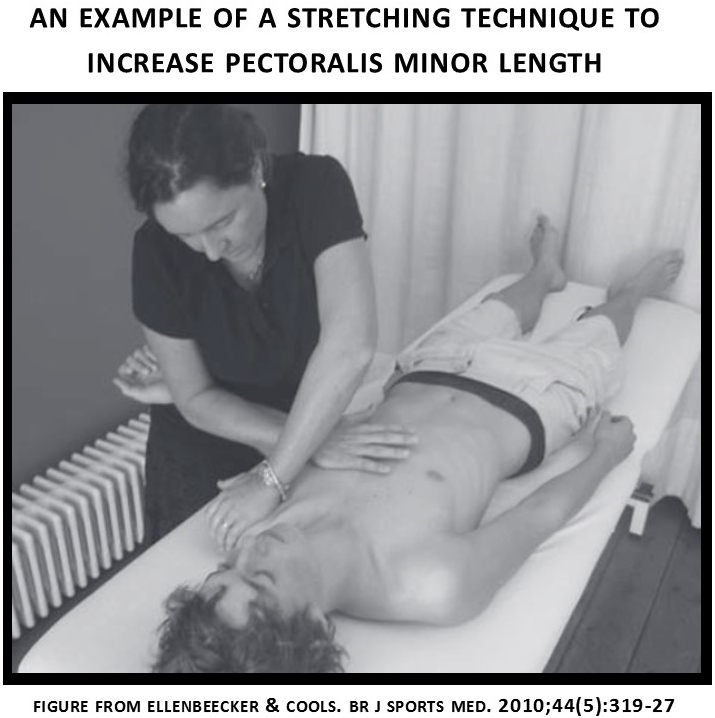
These findings imply that scapular rehabilitation in SIS should be focused on restoring the muscle tone and length of the pectoralis minor rather than performing exercise training which increases the activity of this already overactive muscle. To restore the scapulothoracic muscle balance in SIS patients, stretching techniques of the pectoralis minor are indicated.
Jessica Van Oosterwijck
2016 Pain in Motion
References and further reading:
Castelein B., Cagnie B, Parlevliet T, Cools A. Scapulothoracic muscle activity during elevation tasks measured with surface and fine wire EMG: a comparative study between patients with subacromial impingement syndrome and healthy control. Man Ther 2016;23:33-39. In press but can be previewed on the journal website
http://www.manualtherapyjournal.com/article/S1356-689X(16)00038-2
Ellenbecker TS., Cools A. Rehabilitation of shoulder impingement syndrome and rotator cuff injuries: an evidence-based review. Br J Sports Med 2010;44(5):319-27.
http://www.ncbi.nlm.nih.gov/pubmed/20371557
Struyf F., Nijs J., Baeyens J.P., Mottram S., Meeussen R. Scapular movement and positioning in unimpaired shoulders, shoulder impingement syndrome, and glenohumeral instability. Scand J Med Sci Sports 2011;21:352-358. http://www.ncbi.nlm.nih.gov/pubmed/21385219
{kind=link}
{kind=link}