Invited contribution
It is well established that pain has the function of maintaining the integrity of the body. Pain is an evolutionarily acquired alarm signal of bodily threat and this phylogenetic function is extremely important for survival. It makes sense that pain should automatically demand attention, interrupt ongoing actions, and prioritize appropriate behaviors to escape from bodily threat.
Therefore, pain may have the ability to capture attention. Considering that acute pain is a biologically relevant stimulus, it is expected that it promotes the orientation of attention to the stimulus to adopt rapid behavioral withdrawal from the stimulus. On the other hand, presence of other factors such as negative emotions, catastrophization, anxiety, hypervigilance can draw attention. For example, hypervigilance, which refers to a subject who scans the environment looking for potential threats, selectively engages attention in negative stimulus rather than neutral or positive stimulus.
Patients with continuing pain problems are often assumed to be excessively attentive for their symptoms. It is expected that patients who suffer from chronic pain might associate bodily sensations with danger and display a perceptual habit of scanning the body for threats. This characteristic was described in the fear-avoidance model where a fearful patient becomes more vigilant for signals of bodily threat, which in turn leads to avoidance and disability.
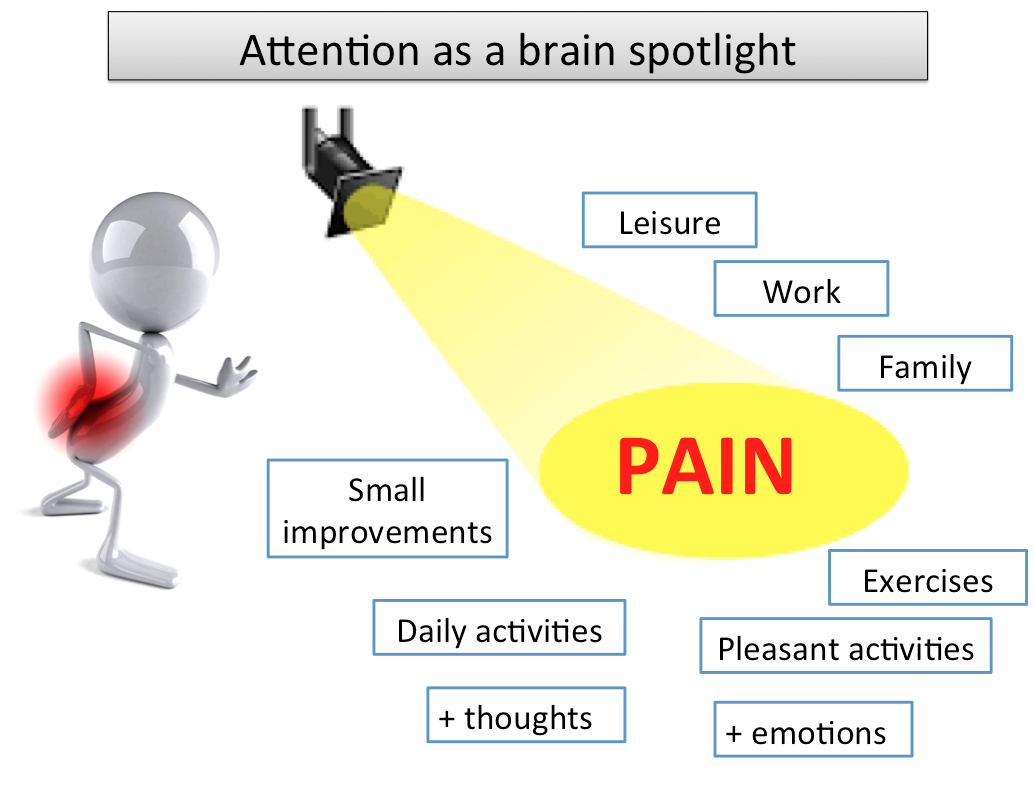
Attention can be compared as a spotlight shading light to a specific stimulus or activity. We drive our attention and select which information will facilitate current goals and ongoing behavior instead of less important demand/stimulus. That ongoing behavior can be interrupted if a more important demand/stimulus emerges. Pain has an interruptive quality because of the activation of a primitive defensive system. For example, imagine that you are seated and working on your computer and suddenly start to experience shooting pain in your leg coming from your lower back. Probably your work will be compromised because your attention now was captured by a painful leg. It means that when we are involved in cognitive tasks or in presence of an emotional stimulus (negative or positive) with a high arousal it is not possible to share attention. Cognitive-emotional interaction is an important brain function and it is expected that cognitive tasks (with a high demand) can regulate an emotional stimulus (for a Review see Pessoa 2015).
There are some therapeutic strategies that can promote emotional regulation and decrease attentional resources to pain. Pain neuroscience education can be understood as an emotional regulation strategy once it aims to decrease negative thoughts, hypervigilance, anxiety, catastrophization and disability. When we explain that chronic pain is not related to the risk of a new injury, patients can drive their attention to a specific goal without focusing on pain. It means that the bottom-up capture of attention to pain can be modulated by top-down activity. Furthermore, pain can be reduced when attention is directed away from the negative stimuli.
However, an important question remains: If it is possible to drive attention away from a painful stimulus (or body part), why do some patients still keep their attention on pain? Why is it so difficult to disengage attention from pain in some patients? The answer may not be related to pain specific but to the personal emotional trait. In an fMRI study from our Conventional and Advanced Neuroimaging laboratory (Sanchez et al.), it was investigated whether individual differences in the positive affect trait modulate attention resources to process unpleasant stimuli. The authors found that participants with a higher positive affect trait exhibited lower amygdala reactivity to unattended unpleasant pictures whereas participants with lower scores showed higher amygdala reactivity. These results suggest that positive affect facilitates the disengagement of attention from the highly unpleasant stimulus.
Considering all exposed until now, there is evidence that attention is preferentially allocated to stimuli that people appraise as threatening or potentially dangerous. Thus, we should consider activities that might facilitate attention disengagement as a cognitive-emotional regulation strategy in patients who suffer from (chronic) pain.
Felipe Reis, PhD
Federal Institute of Rio de Janeiro - IFRJ
Conventional and Advanced Neuroimaging Laboratory (UFRJ)
Pain Research Group (www.pesquisaemdor.com.br)
2016 Pain in Motion
References and further reading:
Sanchez TA, Mocaiber I, Erthal FS, Joffily M, Volchan E, Pereira MG, de Araujo DB, Oliveira L. Amygdala responses to unpleasant pictures are influenced by task demands and positive affect trait. Front Hum Neurosci. 2015 Mar 4;9:107.
https://www.ncbi.nlm.nih.gov/pubmed/25788883
Pereira MG, de Oliveira L, Erthal FS, Joffily M, Mocaiber IF, Volchan E, Pessoa L. Emotion affects action: Midcingulate cortex as a pivotal node of interaction between negative emotion and motor signals. Cogn Affect Behav Neurosci. 2010 Mar;10(1):94-106.
https://www.ncbi.nlm.nih.gov/pubmed/20233958
Okon-Singer H, Hendler T, Pessoa L, Shackman AJ. The neurobiology of emotion-cognition interactions: fundamental questions and strategies for future research. Front Hum Neurosci. 2015 Feb 17;9:58.
https://www.ncbi.nlm.nih.gov/pubmed/25774129
Dalgleish T. The emotional brain. Nat Rev Neurosci. 2004 Jul;5(7):583-9. Review.
http://www.nature.com/nrn/journal/v5/n7/abs/nrn1432.html
Pessoa L. Précis on The Cognitive-Emotional Brain. Behav Brain Sci. 2015
{kind=link}